This section deals with the pathway and the conditions of patients who cannot undergo surgery for either local recurrence or distant metastases, and in whom chemotherapy or other medical therapies are administered in an attempt to curb the progression of the disease.
These conditions usually mean that the disease is incurable.
This is because it is highly unlikely that there are only 1, 2 or 3 metastases in the organism of the patient with advanced cancer. Once metastatic spread has taken place, even if only a few metastases are visible, there will be many others that are still invisible on CT, scintigraphy, PET or magnetic resonance. FIGURE 14
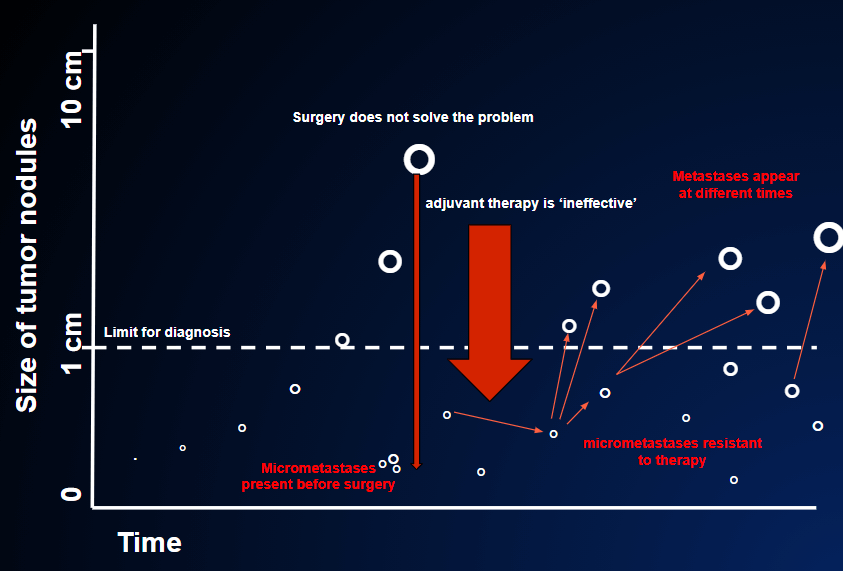
Moreover, even if the visible metastases were surgically removed, the invisible metastases would soon grow and the patient would find himself back in the previous situation, except that now he will have been weakened by a surgical operation that is not usually simple.
So, although it is understandable that patients may pursue the idea of surgery to eliminate metastases, in the vast majority of cases it makes no sense to operate. (WHY SURGERY IS ALMOST NEVER PERFORMED ON METASTASES)
When dealing with metastatic cancer, we generally start with a medical therapy, i.e. drugs that reach the whole organism.
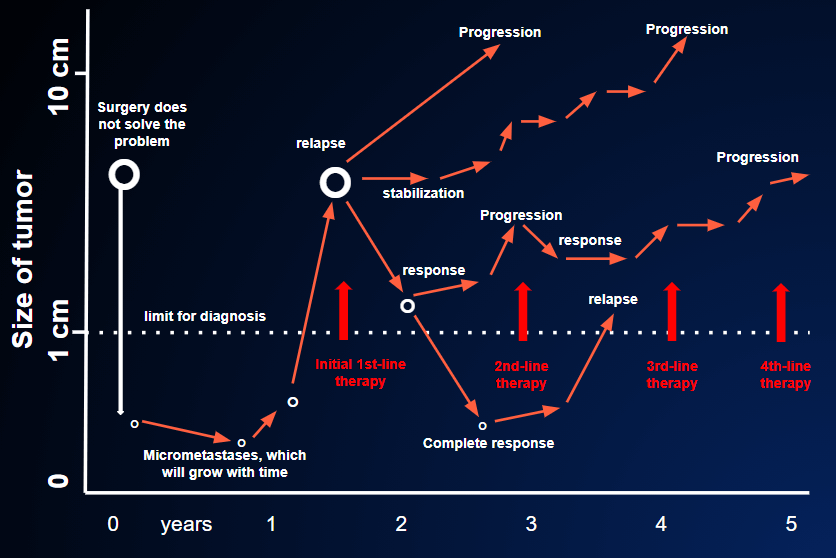
Oncologists use the term “lines of therapy“: the therapy used at the beginning is called the first-line therapy; if this fails, the second-line therapy is administered, and so on. Whether we use chemotherapy, immunotherapy or hormone therapy, the principle is always the same: drugs are administered intravenously, by mouth, or by means of brief or prolonged infusion; these spread throughout the whole body in order to act on the diseased areas.
The aim is to kill the malignant cells, so as to shrink the tumor masses or to block, or at least slow down, their growth. This is what happens if the therapy works; if it does not, the cancer will continue to progress.
Unfortunately, even when the therapy initially works (the tumor shrinks or stops growing), the time will come when the tumor begins to grow again, despite continuation of the therapy. This means that the tumor, which initially responded to the therapy, has become resistant, and the therapy will have to be changed. FIGURE 17
This section on advanced, inoperable cancer is devoted to those patients who:
- begin first-line medical therapies (i.e. therapy is prescribed for the first time) and who are very impatient to fight the growing tumor, which has only recently been discovered; they are at the beginning of the “story” and do not yet know whether the situation will take a more favorable turn, thanks to the therapy, or a less favorable turn;
- obtain only a partial and temporary benefit from the first-line and now see their tumor growing again in spite of the therapy;
- begin second-, third- and fourth-line therapy while their hopes steadily diminish;
- can no longer have any anti-tumor therapy, as it would only be harmful; they therefore receive supportive therapy.
It must be pointed out that, in all of the above-mentioned categories of patients (except the last), surprises can always turn up. Even when the disease seems to have taken a rapid turn for the worse, the therapy may work well enough to elicit new hopes, to put the patient on a more favorable course, and to allow her to enjoy very long periods of worthwhile life, far from hospitals and treatment.