Medical therapies (chemotherapy, hormone therapy, immunotherapy…) are different from surgery and radiotherapy, because they are systemic therapies; in other words, they reach every part of the body, while surgery and radiotherapy act only locally.
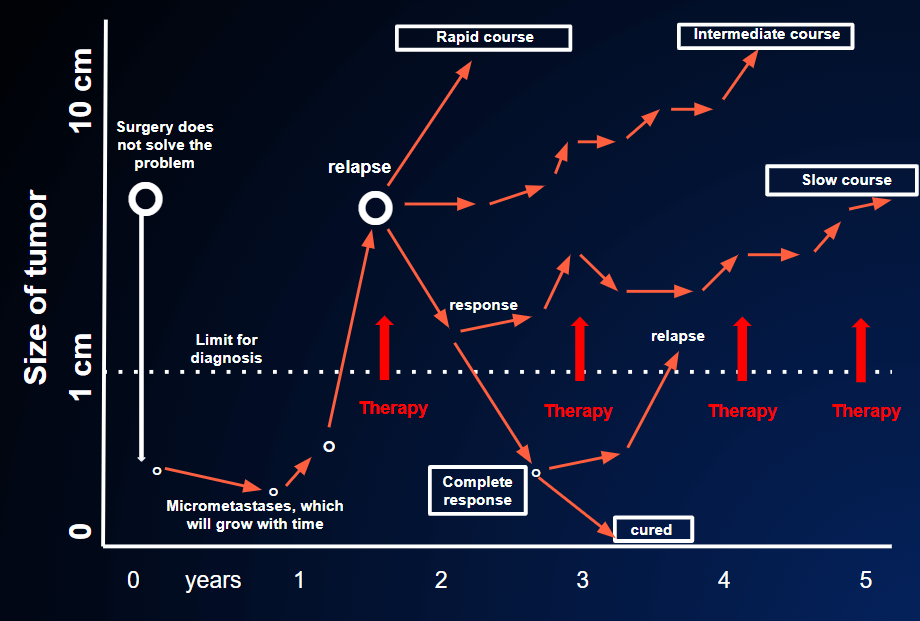
The treatment of metastatic cancer generally begins with the administration of a medical therapy, the aim of which is to shrink the tumor masses or to block, or slow down, their growth. This initial medical therapy is called “first-line” because the patient is at the beginning of the course of the advanced disease. We don’t know yet whether this will work or not, nor do we know what the course of the disease will be like. FIGURE 24
Lines of therapy are not chosen at random. There are precise indications regarding what can and must be used as the first-, second-, third-line therapy, etc. These indications are based on the chances of success, i.e. of a temporary response (reduction in tumor size) to the various treatment regimes. Logically, those regimes that have the greatest probability of success are used first, and are therefore called “first-line” therapies. Subsequently, the effectiveness of the following therapies (second-, third-line, etc) steadily declines.
Radiotherapy also plays a very important role in the treatment of metastases, though it acts only on limited areas of the body (generally a few square centimeters). For example, painful bone metastases, masses that compress vital organs, and symptomatic brain metastases are conditions that can benefit enormously from radiotherapy. For this reason, the treatment of metastases may sometimes begin with a combination of medical therapies and radiotherapy. The medical therapies are aimed at controlling the spread of metastases, while, in the meantime, the radiotherapy acts more radically on critical areas that would impair the patience quality of life in the short term.
Sometimes, radiotherapy is used before medical therapy is started. This happens when there is an urgent need to improve critical local condition (e.g. painful bone metastases that could cause fracture, brain metastases that cause symptoms, etc).
A very important question is “when” treatment should be started. The answer seems obvious. In the vast majority of cases, treatment begins as soon as the diagnosis of metastatic cancer has been made, not least because “hanging around” without taking action causes a lot of psychological stress.
Nevertheless, in some cases the patient’s initial condition does not cause great concern. If the metastases are very small, if the patient is very old and feels well despite having metastases, it may be wiser to wait and see how the disease develops before starting treatment, and then to reassess the situation after 2 months. During this time, the tumor may grow slowly or even remain completely unchanged, and the patient may continue to feel well without undergoing any therapy.
In this way, he can still have a satisfactory quality of life, without being hospitalized or suffering the treatment’s side-effects. Moreover, this delay does not reduce the possibility that the therapy will work once it is started, as long as we don’t wait too long. Indeed, the chances of responding to therapy are no different whether the metastases are 1 cm or 2-3 (WHY WEREN’T THESE METASTASES DISCOVERED SOONER?), though they are certainly lower if the metastases are “massive” (8-10 cm).