After a surgical operation that has, hopefully, eliminated the disease, it must be decided whether or not to administer adjuvant therapy (i.e., preventive therapy). This decision is based on probability and on the balance between: 1) risk, 2) benefit and 3) side-effects. The decision therefore concerns 3 factors.
1. RISK. Once the tumor has been surgically removed, what is the probability of having micrometastases and potentially fatal disease recurrence?
In favorable conditions (a tumor that is not very aggressive and has been removed in its early stages), this risk may be extremely low, about 5%. In such cases, doctors are very unlikely to suggest a therapy that almost always has some side-effects.
with 10-25% risk, the decision to go ahead with the therapy will depend on the possible benefit; if this benefit is about 2-3%, we can discuss the matter; if it is 5-10%, therapy is generally administered
with risk higher than 25-30%, therapy is almost always administered, unless the patient is particularly elderly or frail; even in this latter case, however, the decision will depend heavily on the degree of benefit that can be obtained, which is different in the various tumors.
2.BENEFIT. Is this therapy useful? If so, by how much can it reduce the risk of disease recurrence, given that this risk can never be completely eliminated?
Let’s take the example of a tumor at high risk, about 50%. This means that surgery alone has a 50% probability of curing the disease and a 50% probability of not curing it. If adjuvant chemotherapy is administered, the risk of not curing the disease will be reduced by about 20%. This means that: (FIGURE 8)
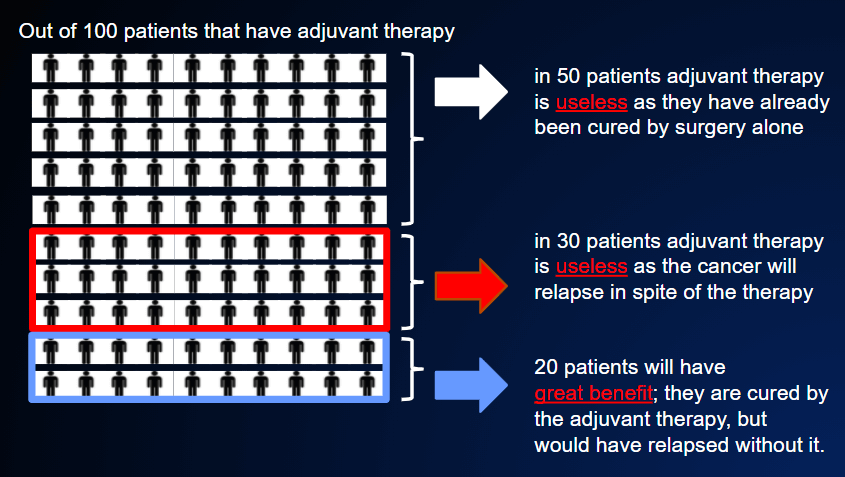
- for 50% of cases, adjuvant therapy has no effect, because the patient is already cured (but cannot know it);
- in 30% of cases, the therapy is useless, as the disease will still recur despite this therapy;
- in 20% of cases, the disease will not recur; the patient will have been cured by this adjuvant chemotherapy, not by surgery.
It is very frustrating that we cannot identify which 20% will be cured by this therapy. If we could, we would be able to avoid administering adjuvant therapy in those 80% of patients in whom it will be useless. Indeed, the search for tests that can distinguish between these two groups is currently one of the most active areas of study.
The table below shows approximate estimates of the average reduction in the risk of relapse in the most common tumors thanks to adjuvant therapy. The percentages shown correspond to the approximate increase in the probability of cure as a result of adjuvant medical therapies, in comparison with surgery alone.
| TUMOR | % REDUCTION IN RISK |
|---|---|
| Breast | 20 |
| colon | 20 |
| rectum | 25 |
| ovary | 25 |
| uterus | 25 |
| Lung | 5 |
| Bladder | 5 |
| stomach | 20 |
| Pancreas | 15 |
These figures are only rough approximations. According to the stage and the risk of each condition, the benefit may vary enormously: from much higher to much lower, or even to zero.
3.SIDE EFFECTS. What is the “price” to pay for adjuvant therapy, in terms of toxicity and discomfort?
In general, the price is fairly high. Chemotherapy is toxic. Although most patients expect to suffer worse side-effects than they actually do, adjuvant chemotherapies are very rarely “light” (they are the same as those used to treat advanced cancer, THE THERAPY IS CAUSING A LOT OF PROBLEMS). This is not the case of hormone therapy, which is generally very well tolerated, even for very long periods (years). Immunotherapy occupies an intermediate position; in most cases, it is very well tolerated, but sometimes it can have very serious toxic effects and need to be suspended.
It is very difficult to predict how severe side-effects will be. The specialist can provide estimates of the intensity and frequency of each possible side-effect, but there is always great variability from one person to another.
To conclude, if adjuvant therapy is prescribed after surgery, it means that:
- the risk of relapse is somewhat high;
- clinical studies conducted over many years have already proved that the therapy proposed is able to reduce this risk;
- the benefits of this therapy far outweigh the possible harm caused by its side-effects.