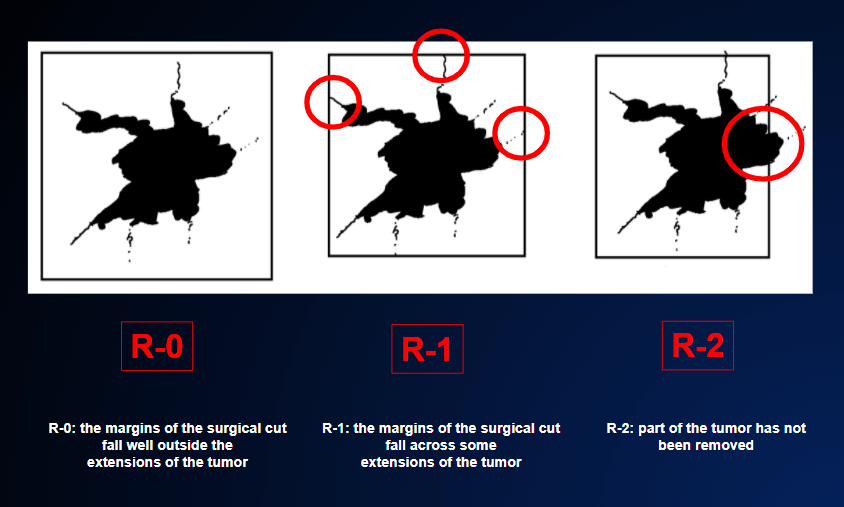
Local recurrence happens because the tumor has not been completely removed during the first surgical operation. This is possible even if the operation is accurately classified as R-0, i.e. complete removal. FIGURE 6 (SURGICAL OPERATION)
But if microscopic examination of the removed tumor shows that the margins of the specimen are tumor-free, how can the tumor re-form in the same place?
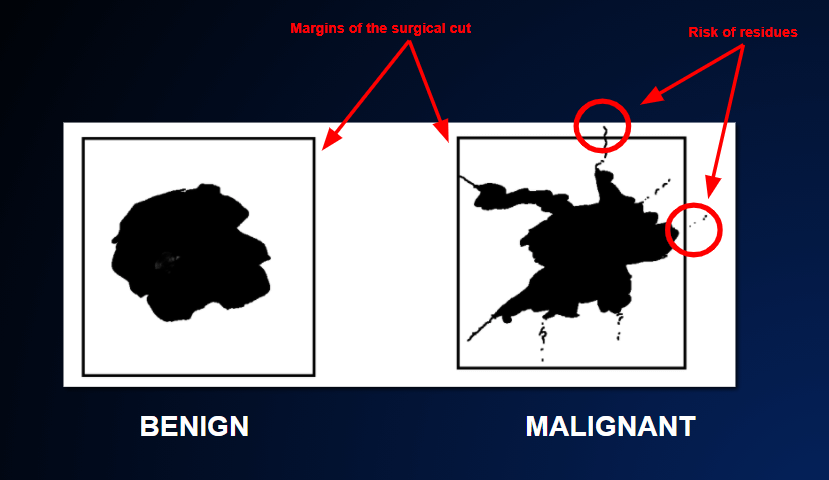
The explanation lies in the fact that a malignant tumor does not grow as a regular nodule, adding layer upon layer (like an onion). Rather, it puts out irregular offshoots from its borders. These offshoots are sometimes extremely fine and invisible to the naked eye. They may even escape observation under the microscope. As these offshoots can even extend for several centimeters, it is possible that microscopic tumor residues may remain in place; even if, “to be on the safe side”, the surgeon removes a layer of 1 or 2 centimeters of healthy tissue from around the tumor. FIGURE 16
One, two or even five years later, these tiny residues of tumor cells may give rise to new tumor masses at the same site from which the tumor was originally removed.
In the event of local recurrence, the hope of cure mainly depends on two factors:
- whether distant metastases have formed between the surgical operation on the primary tumor and the time when the recurrence is discovered. This possibility is immediately investigated, as far as possible, by staging examinations (CT, PET, magnetic resonance…).
- whether the local recurrence is limited and can therefore still be removed. In theory, if the recurrence is localized, it should always be possible to remove it. In reality, however, it is often impossible to remove it; this is the case when the tumor is very close to vital organs that cannot be surgically removed.
In the case of a local recurrence in a breast that has undergone partial mastectomy some time ago, it is fairly obvious that complete removal of the rest of the breast will offer a very good chance of cure.
In cases of tumors of the lung, stomach, bladder, uterus or rectum, however, the scenario is very different. Indeed, in such cases, a large amount of the surrounding tissues and nearby structures will already have been “sacrificed” during surgery to remove the primary tumor. This means that, in most cases, the local recurrence does not leave room for further surgery. Moreover, there would be no point in removing only a part of the new tumor mass (so-called R-2 resection) FIGURE 6, as the part left in place would rapidly regenerate. Indeed, this incomplete removal sometimes accelerates the growth of the tumor, as the cut made by the scalpel favors the release of several tumor growth factors.
In this regard, it is advisable to consult a team of experts in “difficult” cases of local recurrence, as the chance of cure (albeit slim) is at stake. Surgeons, with radiologists and oncologists, consider all possible ways to eliminate the recurrence completely. If it cannot be removed completely, the tumor can only be controlled temporarily; unfortunately, it will progress over time and spread to other organs.